Healthcare recruitment strategies: 13 ways to hire healthcare professionals faster in 2026
Filling one experienced RN role takes 78 days on average, according to the 2026 NSI National Health Care Retention Report. A caregiver, meanwhile, is often off the market within three days of applying.
This guide covers 13 healthcare recruitment strategies for in-house hiring teams at clinics, hospitals, and home care organizations.
You'll get the channels that actually produce clinical candidates, a screening setup that handles volume, and the retention math that stops you from refilling the same roles every quarter.
One thing to know up front: most of what ranks for this topic is written by staffing agencies selling placements. This is the playbook for doing it yourself.
Key takeaways
The hiring playbook, in your inbox
One email a week - benchmarks, AI screening tactics, and short interview templates from the 100Hires team. No product pitches.
- Publish real pay and real conditions. Vague postings filter out the good candidates, not the bad ones.
- Indeed, niche boards, and referrals beat LinkedIn for clinical roles.
- Speed wins. Caregivers and nurses accept the first credible offer, so respond in hours, not days.
- Screen candidates with knockout questions at the application stage instead of reading resume piles.
- Retention is recruiting. Most healthcare hiring pain is the same roles turning over again and again.
Why recruitment in healthcare is harder than in any other industry
The numbers explain why your open roles feel harder to fill every year. The Bureau of Labor Statistics projects about 1.9 million openings in healthcare occupations every year through 2034.
Home health and personal care aides add more new jobs than any other single occupation in the country.
Demand keeps growing. Supply does not keep up.
The 2026 NSI report, built on data from 527 hospitals, puts staff RN turnover at 17.6% and the cost of one RN departure at $60,090. The average RN vacancy sits open for 78 days, and some hospitals report over 100 days.
Physicians are no easier. The AAMC projects a shortfall of up to 86,000 physicians by 2036, and a fifth of practicing physicians are already 65 or older.
Here's the part most hiring content skips: the pipeline is capped upstream. Nursing schools turned away 65,766 qualified applications in 2023 alone for lack of faculty and clinical placements, per the American Association of Colleges of Nursing.
Peer-reviewed research on healthcare workforce recruitment reaches the same conclusion: you're competing for a pool that cannot quickly grow.
So every strategy below does one of three things. It widens your funnel, moves you through it faster than the org down the street, or shrinks the number of hires you need in the first place.
13 healthcare recruitment strategies for clinics, hospitals, and home care
One principle before the list: recruiting volume means nothing if the same roles reopen every quarter. Fixing the leak is strategy 10, and it's the one that shrinks next year's requisition load.
The list runs from tactics you can apply this week (postings, channels, speed, screening) to the structural plays that compound over years (pipelines, internal mobility, role-specific playbooks).
1. Publish real pay, real conditions, and benefits that solve life constraints
Healthcare candidates have seen enough postings to read between the lines. In one r/physicaltherapy thread, clinic owners asking how to hire PTs got the same answer over and over: "competitive wages" reads as a warning label. Experienced clinicians skip those listings entirely.
Sign-on bonuses get the same treatment. Nurses discussing a $30k bonus openly advised each other to look past the headline number and shop around, since a big bonus with hidden ratios usually means a unit nobody stays in.
What to publish instead: the exact pay range, the shift pattern, patient ratios where they apply, and a day-in-the-life paragraph written by someone who does the job.
Postings with real staff photos and stories pull more inquiries than text-only listings, per recruiters at Cherry Health who run physician searches for a living.
Benefits work best when they solve life logistics for shift workers: child care and back-up care, tuition support, education pathways, schedule flexibility. Those retain people long after a one-time bonus is spent.
Pay-transparency laws are spreading anyway. Publish before it's mandatory, and get credit for it while it still reads as a choice.
2. Go where clinical candidates actually are (it's usually not LinkedIn)
This one contradicts most recruiting advice. Healthcare recruiters on Reddit, our own sales calls with clinics, and practitioner videos all say the same thing: most nurses, caregivers, and techs don't maintain LinkedIn profiles.
LinkedIn earns its keep for leadership and admin roles only.
Where clinical candidates actually show up:
- Indeed - the volume leader for RNs, CNAs, and medical assistants.
- Healthcare-specific boards - HospitalRecruiting, HealtheCareers, and vertical nurse boards reach people general boards miss.
- State license boards - lists of verified, currently licensed professionals with far less recruiter competition.
- Facebook groups - regional and specialty groups outperform LinkedIn for clinical outreach.
- Schools and certification programs - the entry-level pipeline for CNAs, MAs, and techs.
Track cost and conversion per channel before renewing any board contract. Manual posting runs $30-50 per day per board, a figure our clinic customers confirm on sales calls.
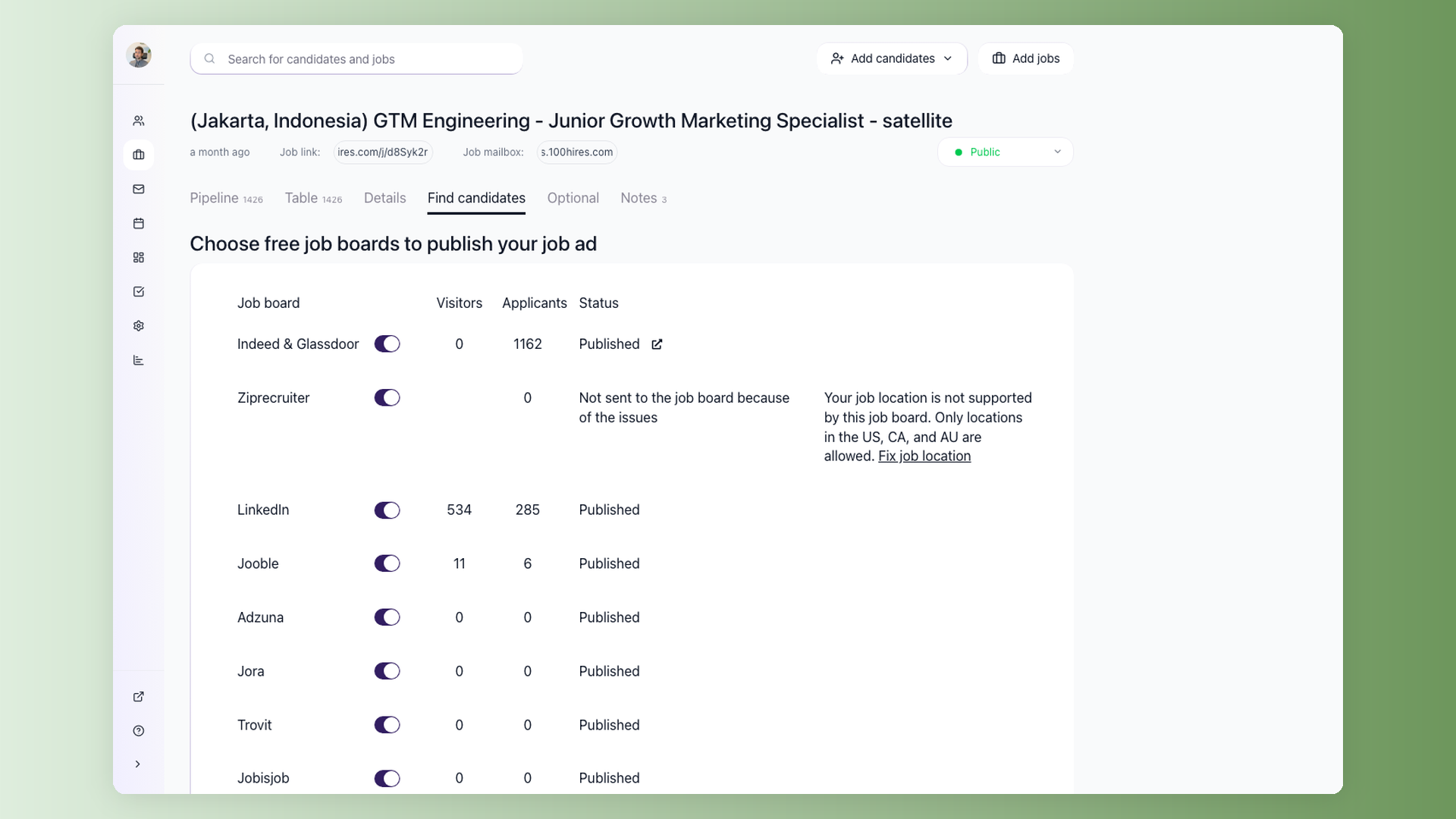
An ATS with multiposting pushes one job to 1,000+ boards in a click and lands every applicant in one pipeline.
3. Respond in hours, not days
Speed is the cheapest competitive advantage in healthcare hiring. Activated Insights reports that over half of caregivers can start a new role within about three days. The first credible responder usually wins them.
The competition moves fast too. A Canadian clinic recruiter described posting a single locum opening and watching 20-30 competing recruiter messages reach the same physicians within 24 hours. Standard offer windows in nurse hiring run about a week before the candidate moves on.
Four habits compress your response time: screen new applicants the same day they apply, let candidates book their own interviews with self-scheduling links, set a decision deadline for every pipeline stage, and pre-approve compensation so an offer never waits on a committee.
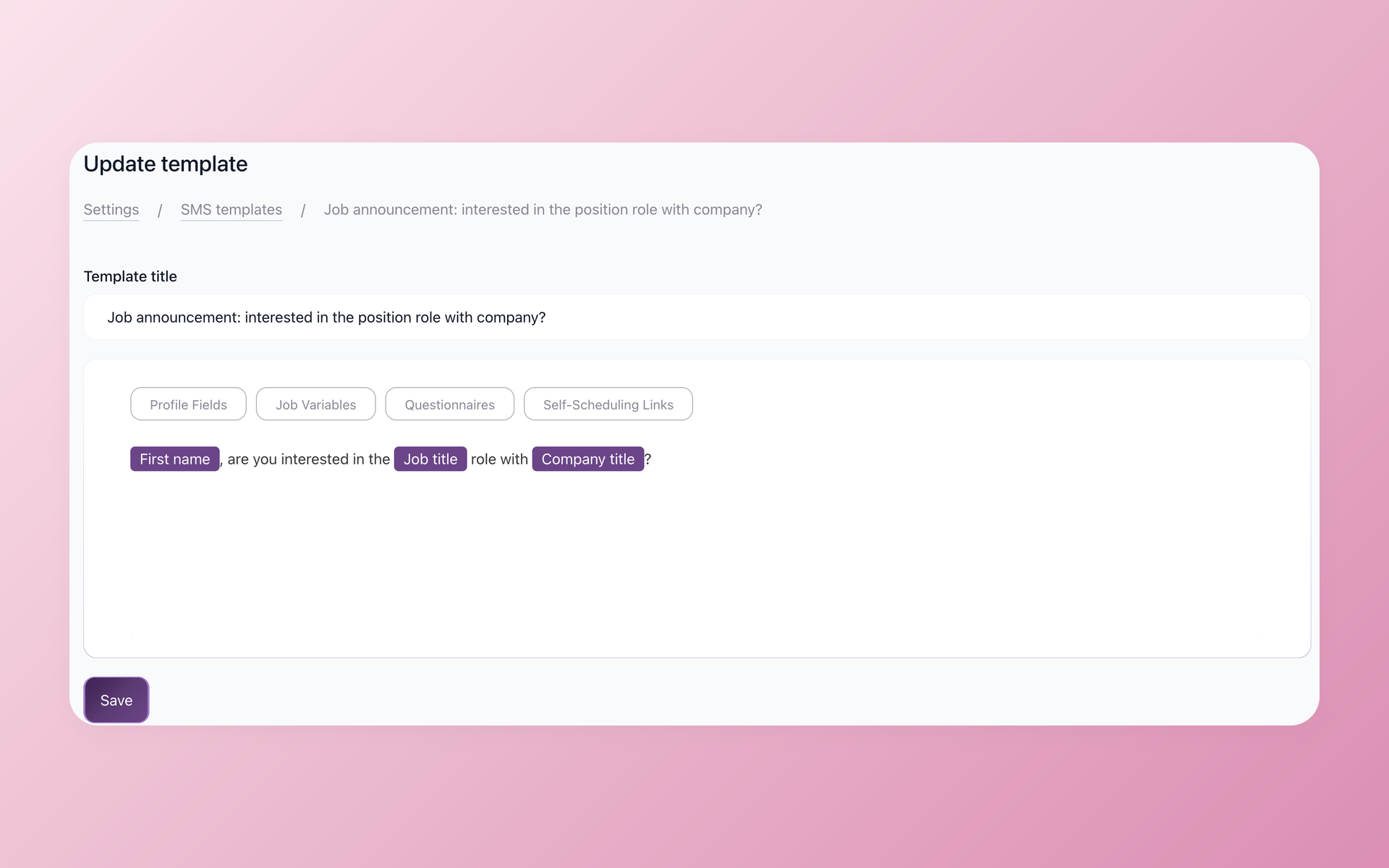
4. Text candidates around their shifts
Clinical staff work 12-hour shifts. Daytime calls and emails land when they physically cannot answer, which is why healthcare recruiters on r/recruiting describe timing texts to hit near shift-end and getting replies within hours.
Email has a second problem at volume. One healthcare facility we demoed for had been blasting nurse lists through MailChimp and kept tripping spam flags, since marketing tools treat cold recruiting email as abuse.
Text recruiting through an ATS logs every exchange on the candidate record and adds call forwarding, so a returned call reaches a human instead of voicemail.
Keep messages short and concrete: role, pay, location, one question. That's it.
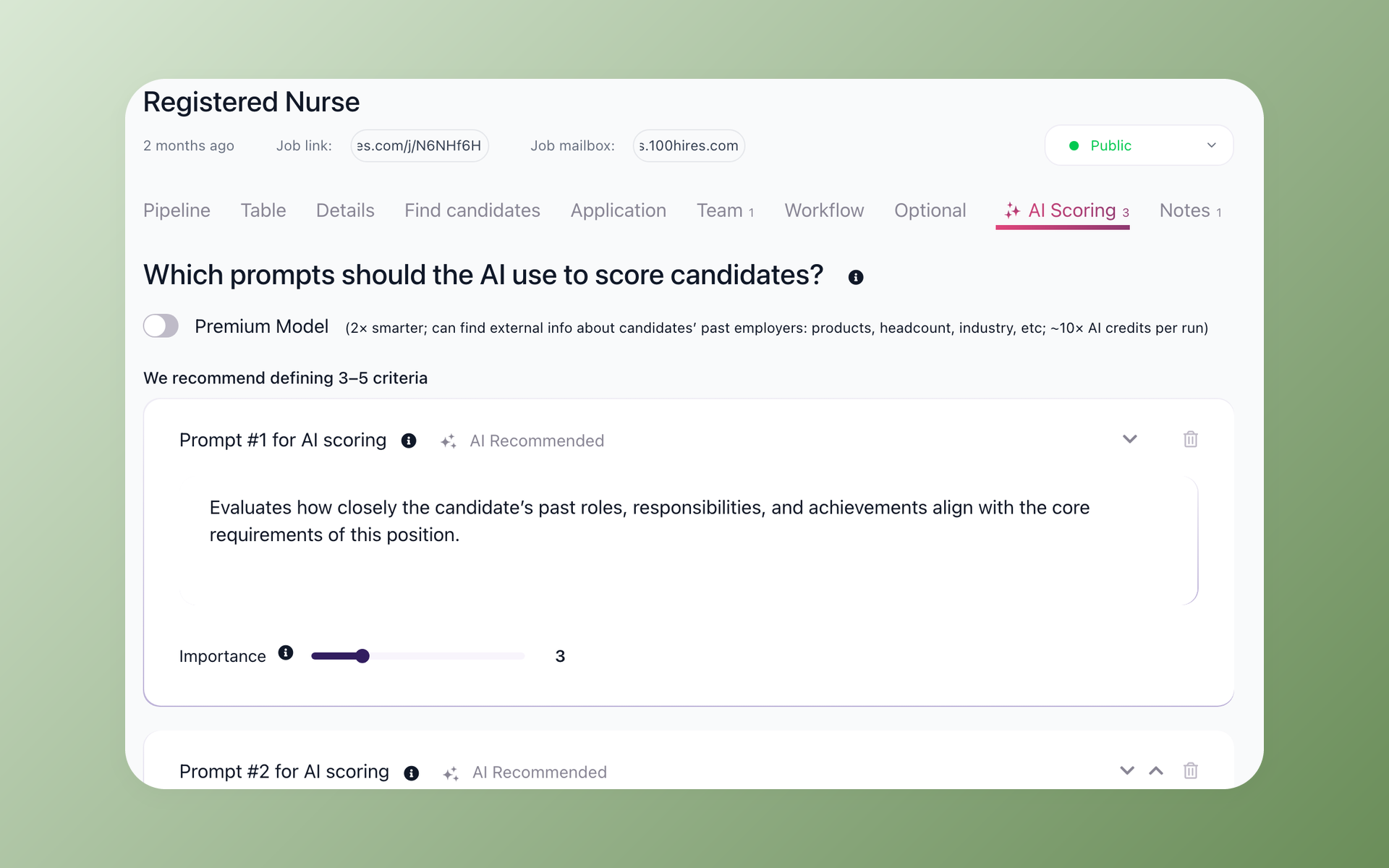
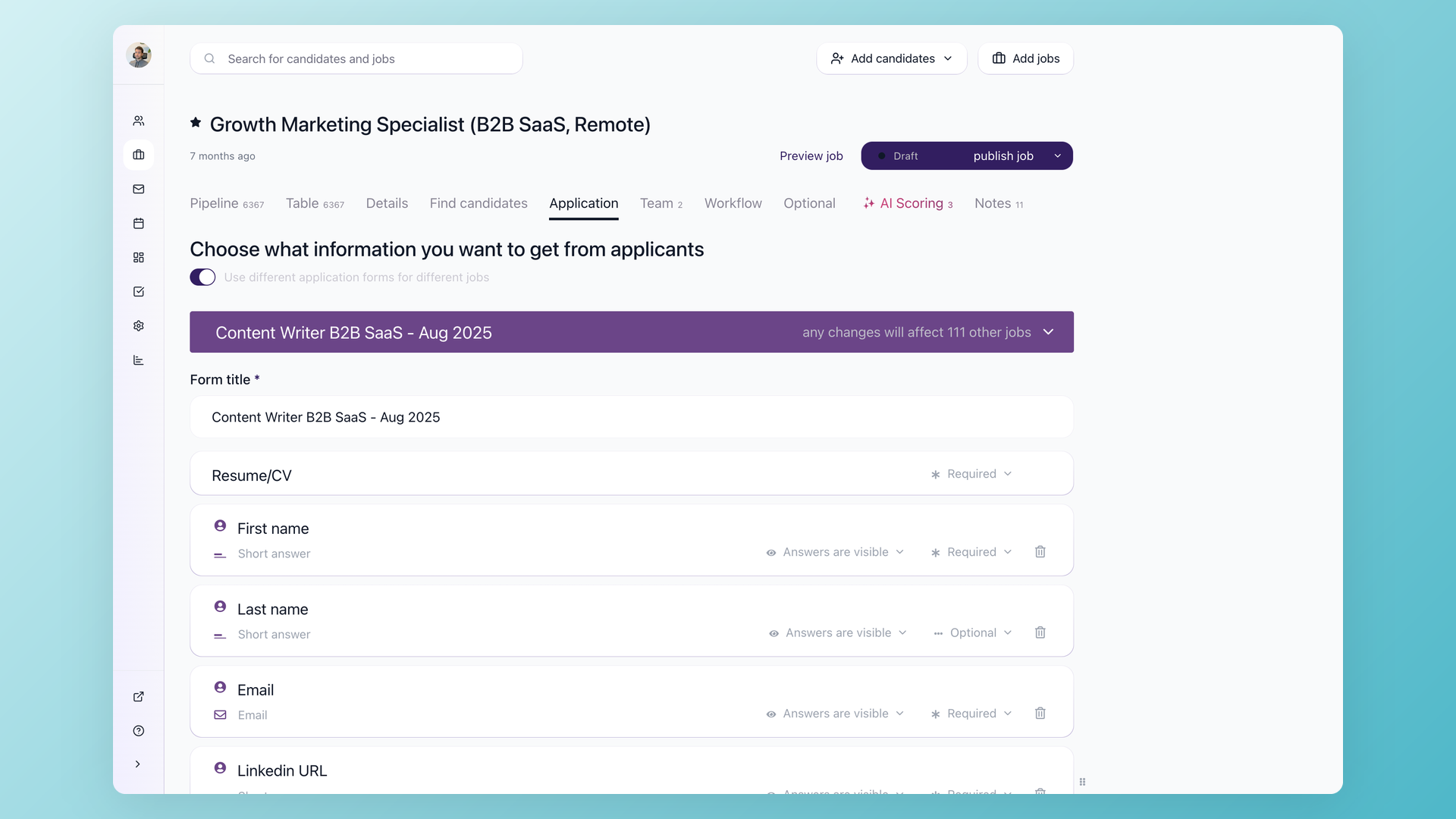
5. Screen with knockout questions at the application stage, and keep the form short
Application volume isn't the bottleneck. Triage is. A VP of clinical operations described getting 250 applications in 48 hours for one remote clinical research role. Two full days went to resume review, and 11 people made the shortlist.
Home care sees the same funnel shape: the median agency turns roughly 800 applicants into 63 hires, per HHAeXchange's analysis of Activated Insights benchmarking data.
The fix is screening at the moment of application. Knockout questions on license type, certification, availability, transportation, and commute radius disqualify mismatches instantly.
AI scoring ranks whoever clears the gate, so reviewers start from the top instead of reading 800 resumes in order.
Keep the form itself short: a 2-3 minute mobile application that asks only the essential knockout questions.
Send the longer questionnaire automatically after candidates apply, but only to those who already passed. You keep the screening data without losing applicants to a ten-page form.
One judgment call from a real medical practice: a candidate with 15 years of experience but a lapsed certification shouldn't be auto-rejected. Route edge cases to manual review instead of a hard knockout.
Full disclosure: 100Hires is our product, and it implements this exact pattern with knockout questions, AI Score, and post-apply questionnaires. Most modern ATSs offer some version - the strategy stands whichever vendor you pick.
If you're comparing tools, the healthcare recruiting software page walks through the clinic setup.
6. Embed license and credential verification into every stage
Healthcare hiring dies in credentialing queues. License class and state, certifications, background checks, work-authorization paperwork - each one stalls an offer when it's handled ad hoc.
Build verification into the pipeline itself. Confirm license class at the application with a knockout question. Make the background check a defined stage that fires an automated email to the candidate with instructions, instead of someone remembering to send it.
Keep an audit trail of who verified what and when; our guide to recruitment compliance covers what a defensible record looks like.
Direct care adds a work-authorization layer. KFF analysis puts immigrants at roughly 30% of the US direct care workforce, so I-9 discipline is ongoing process hygiene, not a one-time checkbox.
Use the EEOC-safe question ("Are you legally authorized to work in the US?") and leave it at that.
7. Build a referral engine, not a referral policy
Home care operators in two separate Reddit communities, including this home-care HR thread, independently described the same pattern: their referral hires stayed roughly twice as long as job-board hires.
Practitioner surveys shared by nurse-recruitment specialists put referrals in the top two reasons nurses apply anywhere.
Most orgs have a referral policy. Few have an engine.
The difference: bonuses paid in tranches tied to the referred hire's tenure, a submission flow that takes under a minute, the whole team trained to spot recruiting moments (not just HR), and referral wins publicized internally so the habit spreads.
One caveat from the same operators: referral quality collapses if you're simultaneously mass-hiring anyone who applies. Your best staff stop vouching for a workplace that hires warm bodies.
8. Treat your careers page like a patient-acquisition landing page
Healthcare marketing teams A/B test every patient acquisition page and leave the careers page as a job list with a form. Recruitment marketers who fixed this at large health systems recommend running it like any conversion asset.
The checklist:
- A real value proposition, not a list of openings
- Video testimonials from current staff
- Dedicated sub-pages for benefits and PTO (candidates expect a page per topic)
- A live job feed from your ATS instead of a stale list
- A content refresh every quarter
- Scroll tracking to see what candidates actually read before applying
If your retention beats the industry average, say so on the page with the number. It's an underused trust signal.
9. Re-engage the candidates and staff you already know
The cheapest sourcing pool is people who already know you.
In a recorded interview, WellSpan Health's recruitment marketing lead described a win-back campaign for nurses who'd left within three years: hiring managers called personally, postcards with QR codes followed a week later.
It helped drive a record month of roughly 9,100 applications across the system.
The same team geofenced digital ads around one specialty conference for about $4,000 and landed 20+ hires - against six-figure search-firm fees for a single placement in those specialties.
Your silver-medal candidates deserve the same treatment. Every screened near-miss goes into a talent pool with a periodic check-in, so a reopened role starts from a warm list instead of zero.
In 100Hires, Nurture Campaigns run those check-ins automatically and pause the moment a candidate replies.
10. Fix retention so you stop refilling the same roles
Now the leak itself. Median caregiver turnover runs about 75% a year, and about 57% of it happens in the first 90 days, per HHAeXchange's analysis of Activated Insights benchmarking data. Onboarding isn't paperwork. It's a retention intervention.
What the first 90 days should include: a structured plan ready before day one, a named preceptor or mentor, and a shadow day before the offer is accepted so expectations match reality.
Nurse recruiters at two DC-area hospitals independently credit residency programs with better first-year retention among new grads.
For caregivers, the retention lever is scheduling density. Operators who pushed turnover below 40% describe the same move: give people full weeks within a tight radius instead of fragmented shifts across town.
Internal float pools and PRN tiers absorb census swings without burning out the core team or defaulting to agency spend.
And a harder truth from TA leaders on LinkedIn: facilities that can never keep roles filled usually have a culture or investment problem that persists across market cycles. No recruiting tactic outruns that.
11. Partner with schools before you need the graduates
The nursing shortage is partly a training-capacity problem. Per AACN data, nursing programs turn away tens of thousands of qualified applications a year - not for lack of interest, but for lack of faculty and clinical placement slots.
Employers who host clinical placements get first look at every graduating class.
The rest of the playbook: tuition assistance tied to tenure, CNA-to-LPN-to-RN ladders, and growing your own educators - your bedside nurses with three to five years of experience are already precepting informally and can teach part-time.
For physicians, placement stints work the same way. Recruiters treat locum and residency placements as a permanent-hire pipeline, since physicians tend to put down roots where they first practice.
12. Unblock internal mobility before hiring externally
Here's the strategy no listicle mentions. In a heavily upvoted r/nursing thread, nurses described unit managers quietly blocking internal transfers to protect their own headcount.
The org then hires new grads externally and concludes it "can't find experienced nurses" - a sourcing problem that is actually an internal politics problem.
The fixes are policy, not sourcing: transparent internal posting rules, a service-level deadline on transfer decisions, backfill budgets so a releasing manager isn't punished for saying yes, and internal-mobility metrics reviewed at leadership level.
Internal hires already know your systems and stay longer.
13. Match the playbook to the role
Physician, nurse, and caregiver hiring are three different problems wearing one label. No in-house guide in the search results splits them, so here's the short version.
Physicians: recruiters who do this full time describe 3-12 month cycles. Do deep intake before any outreach - call schedule, patient population, team size - since a physician who can't get answers to their first two questions disengages.
Plan on three to four touches with five to seven days between them.
Spousal employment and cost of living decide relocations, and rural sites win by selling the area and lifestyle, not just the job.
Nurses: Indeed plus referrals plus residency programs. Speed and schedule transparency help you win candidates. Publish the unit and the ratios.
CNAs, caregivers, and home care: the segment where BLS projects the most new jobs of any occupation. Mobile-first short applications, texting as the default channel, and a hard focus on the 90-day cliff.
Wage pressure here is structural - reimbursement policy caps what agencies can pay - so compete on schedule density and candidate experience. We cover this segment's playbook in depth on our home care recruiting software page.
Common healthcare recruiting mistakes to avoid
- Warm-body hiring. Every 30-day flame-out costs a replacement hire and burns out the staff who covered the shifts. It feeds the exact turnover loop you're recruiting against.
- Bonus-first postings. A big sign-on number with hidden ratios and schedule reads as bait. Candidates warn each other about these listings by name.
- "Competitive wages." Publish the number or lose the experienced applicants who refuse to waste three interviews finding it out.
- Defaulting to LinkedIn. That's where corporate recruiting lives, not where clinical candidates live.
- Blaming ghosting on candidates. Both sides ghost. The fix on your side is speed and confirmed next steps, every stage, every time.
- Buying volume before fixing triage. More job-board spend on top of a broken screening process just relocates the bottleneck to your inbox.
When should healthcare recruiting move from spreadsheets to an ATS
Run the math on the median home-care funnel: roughly 800 applicants for 63 hires a year, per HHAeXchange. Reading every applicant at two minutes each is about 27 hours a month of resume review.
Add $30-50 per day per job board, per role, and a spreadsheet that someone maintains by hand.
We've watched this on sales calls: one nurse recruiter was juggling about 100 candidates in Excel with email reminders, and the system fell apart exactly when hiring picked up.
| Hiring step | With 100Hires | Manual process |
|---|---|---|
| Screening | Knockout questions + AI Score filter and rank on arrival | Read every resume, ~27 hours/month at median volume |
| Job board distribution | One click to 1,000+ boards, one pipeline | $30-50/day per board, posted and tracked by hand |
| Outreach | SMS and email sequences that pause on reply | Individual calls and emails during shifts candidates can't answer |
| Scheduling | Self-scheduling links, candidate books instantly | Email tag across days |
| Tracking | Every candidate, note, and text stored in one record | Spreadsheet rows and memory |
Where 100Hires stops: it's a recruiting workflow tool, not shift-scheduling, EVV, credentialing, or payroll software. And no ATS fixes a pay or culture problem - strategies 1 and 10 are on you.
Pricing starts at $49/month billed annually, compared with enterprise healthcare platforms that typically run several hundred per month. You can start a free trial or book a demo and have a working pipeline the same afternoon.
FAQ
How long does it take to fill a healthcare position?
An experienced RN role takes 78 days on average (range 56-102), per the 2026 NSI National Health Care Retention Report. Physician recruiters describe search cycles of 3-12 months, and caregivers often move in days. Most organizations reclaim weeks in the screening-to-interview gap - in 100Hires, knockout questions plus self-scheduling links let a qualified applicant book an interview the day they apply.
What is the most effective healthcare recruitment strategy?
No single channel wins alone. Operators consistently report referral hires staying far longer, Indeed produces volume, and response speed multiplies everything else. The practical move is measuring which channel converts before renewing spend - 100Hires Trackable links show visitors, candidates, and conversion rate per source, so the budget follows evidence.
How to recruit healthcare professionals for hard-to-fill roles?
Go passive: source from state license boards, join regional and specialty Facebook groups, run drip outreach with five to seven days between touches, and geofence ads around specialty conferences. Persistence matters more than volume: physician recruiters say responses often come on the third or fourth touch. 100Hires Nurture Campaigns run that drip automatically and pause the moment a candidate replies.
How do you recruit and retain healthcare professionals?
Treat them as one system. Structured 90-day onboarding, residency programs, and schedule density keep the people you hire, and retention shrinks next year's recruiting load - about 57% of caregiver turnover happens in the first 90 days, per HHAeXchange. On the recruiting side, 100Hires Talent Pools re-engage past candidates so a reopened role starts warm instead of from zero.
How is recruitment in healthcare different from other industries?
Three structural differences: candidates are license-gated (you screen credentials, not just experience), they work 24/7 shifts that break email-first outreach, and the talent supply is capped by training capacity rather than interest. That's why 100Hires builds knockout questions around license, certification, and availability - the screening healthcare actually requires.
How can a small clinic compete with hospital systems for talent?
Beat them where they're slow: respond the same day, publish exact pay, offer schedule transparency a large system can't match, and sell community and lifestyle for rural sites. Targeted low-cost campaigns outperform brand budgets at clinic scale. 100Hires starts at $49/month billed annually, which puts a full hiring workflow inside a clinic budget.
Start with the leak, then the funnel
The order of operations: post honestly, pick the channels clinical candidates actually use, move faster than the org down the street, screen at the application, and keep the people you hire. Each strategy compounds the others.
If your current process is a spreadsheet and a stack of browser tabs, that's the first fix. Start a free 100Hires trial and set up knockout questions, multiposting, and texting on your next opening.
Try 100Hires for free
No credit card. 14-day trial. Forbes Advisor #1 ATS for SMBs.
